Dementia Fall Risk for Beginners
Dementia Fall Risk for Beginners
Blog Article
A Biased View of Dementia Fall Risk
Table of ContentsDementia Fall Risk Can Be Fun For AnyoneDementia Fall Risk Can Be Fun For EveryoneThe Buzz on Dementia Fall RiskAn Unbiased View of Dementia Fall Risk
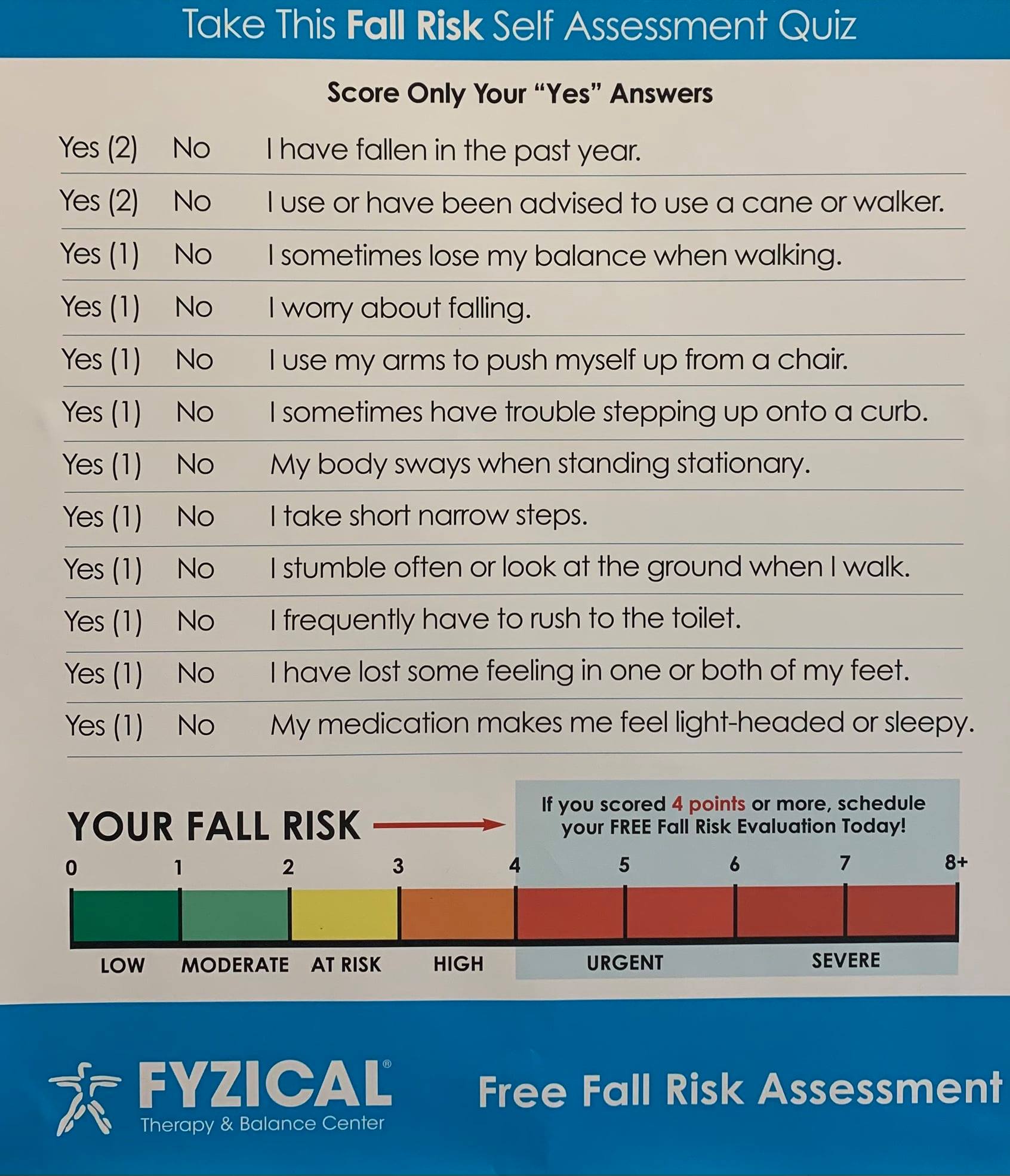
A fall risk analysis checks to see just how likely it is that you will fall. The evaluation typically consists of: This consists of a collection of inquiries concerning your total health and if you've had previous falls or problems with equilibrium, standing, and/or strolling.Interventions are recommendations that might decrease your threat of falling. STEADI includes three actions: you for your danger of dropping for your risk elements that can be boosted to attempt to stop drops (for instance, balance problems, damaged vision) to minimize your danger of dropping by making use of effective strategies (for instance, offering education and sources), you may be asked numerous questions including: Have you dropped in the past year? Are you fretted regarding dropping?
You'll rest down once more. Your provider will check the length of time it takes you to do this. If it takes you 12 seconds or more, it may indicate you are at greater threat for a fall. This test checks stamina and balance. You'll sit in a chair with your arms went across over your upper body.
The settings will get more difficult as you go. Stand with your feet side-by-side. Move one foot halfway onward, so the instep is touching the large toe of your various other foot. Move one foot fully before the other, so the toes are touching the heel of your various other foot.
Dementia Fall Risk Fundamentals Explained
The majority of drops take place as a result of multiple contributing elements; consequently, managing the risk of dropping begins with determining the factors that add to drop danger - Dementia Fall Risk. Several of the most relevant danger aspects include: Background of previous fallsChronic medical conditionsAcute illnessImpaired stride and equilibrium, reduced extremity weaknessCognitive impairmentChanges in visionCertain risky medicines and polypharmacyEnvironmental aspects can likewise increase the danger for drops, consisting of: Inadequate lightingUneven or harmed flooringWet or unsafe floorsMissing or damaged hand rails and get barsDamaged or poorly fitted devices, such as beds, wheelchairs, or walkersImproper use assistive devicesInadequate guidance of the people staying in the NF, including those who display hostile behaviorsA successful loss risk monitoring program requires a detailed professional analysis, with input from all participants of the interdisciplinary team
.png)
The treatment plan should also consist of treatments that are system-based, such as those that advertise a risk-free atmosphere (appropriate lighting, hand rails, grab my website bars, etc). The efficiency of the treatments should be assessed regularly, and the care strategy changed as required to show modifications in the autumn threat analysis. Carrying out a loss risk administration system using evidence-based ideal technique can decrease the frequency of falls in the NF, while limiting the possibility for fall-related injuries.
An Unbiased View of Dementia Fall Risk
The AGS/BGS standard suggests screening all grownups aged 65 years and older for fall danger yearly. This screening is composed of asking patients whether they have fallen 2 or more times in the past year or looked for medical interest for an autumn, or, if they have not dropped, whether they feel unsteady when walking.
People that have actually dropped once without injury should have their balance and stride assessed; those with stride or equilibrium irregularities ought to get added analysis. A background of 1 fall without injury and without gait or balance problems does not call for additional assessment beyond ongoing yearly fall danger screening. Dementia Fall Risk. An index autumn threat analysis is called for as component of the Welcome to Medicare assessment
The Best Guide To Dementia Fall Risk
Documenting a drops background is one of the quality indicators for autumn avoidance and administration. A critical component of risk evaluation is a medication review. Numerous courses of medications raise loss threat (Table 2). copyright drugs particularly are independent predictors of falls. These medications often tend to be sedating, modify the sensorium, and hinder equilibrium and gait.
Postural hypotension can frequently be eased by reducing the dosage of blood pressurelowering medications and/or stopping medicines that have orthostatic hypotension as a negative effects. Usage of above-the-knee support hose pipe and copulating the head of the bed boosted might also decrease postural decreases in high blood pressure. The suggested components of a fall-focused physical assessment are displayed in Box 1.
A TUG time better than or equivalent to 12 seconds suggests high loss threat. The 30-Second Chair Stand test evaluates lower extremity stamina and equilibrium. Being not able to stand from a chair of knee elevation without making use of one's arms shows increased loss risk. The 4-Stage Equilibrium test evaluates fixed balance by having the person stand in 4 positions, each considerably much more difficult.
Report this page